



Pexels—Image by Ivan Siarbolin
Take a moment to think about the last week in your practice. What did you talk about? How did it feel?
If one of your clients struggled with anxiety, what is your understanding of what anxiety “is” and why it shows up? What kinds of interventions do you rely on when people are too anxious to cope?
If a client told you she was flooded with memories from a trauma and there was no clear trigger for the memories, what did you assume was causing the problem? What was your first question, and what did you think would help?
If you gave a person homework, did you ask them to fill out a worksheet, keep a log, track a mood, experiment with a new behavior, or challenge a rehearsed pattern of thinking? Did you ask them to take a yoga class, or practice meditation, or immerse themselves in the woods?
How do you generally start a session? Do you ask about a person’s recent experiences? Do you focus on their habitual thoughts? Their sleep patterns? Their levels of emotional and physical pain?
Do your clients regularly tell you about their experiences of embodiment? When they talk about their bodies, where do they focus their attention?
If you were the one in therapy, did you talk about your body—how it works, what it does, what you think about it, how it feels to inhabit it?
The understanding of what a body “is” and how it works shapes the interventions we are trained to use and how we think about psychological distress. There are at least three definitions of the body driving today’s mental health treatments, and these definitions are creating unofficial silos in the field, parceling out different understandings of embodiment and selfhood.
In some forms of therapy, the mind, or consciousness, is addressed as if it is detached from the body. In some, our distress is thought to be rooted in the body’s systems, or in the brain’s functions. In others, the body’s affect or arousal is thought to drive the person’s thoughts and behaviors. And in others, the experience of embodiment is thought to be inextricable from culture, which gives us the language and the meaning systems that shape our sense of self.
This is obviously a huge topic, so for today, I’m going to outline these three definitions of the body and talk about how they are driving different interventions for healing mental distress. In future posts, I’ll come back to these ideas so we can start talking about what embodiment “is” in mental health.
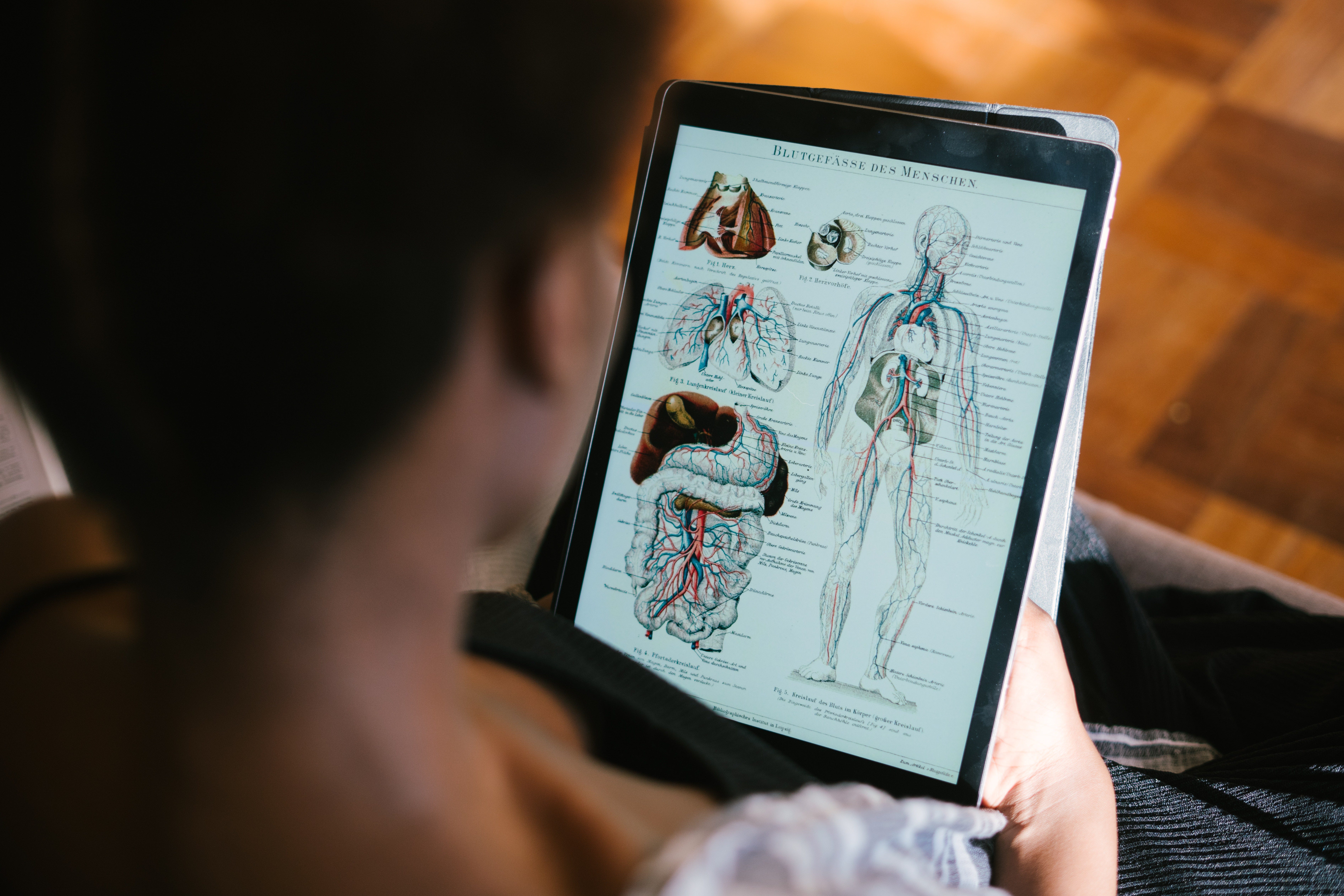
The physiological body
Pexels—Image by RF._.studio
This definition of the body is the one that we commonly associate with medicine. Mental health treatments that are derived from brain research are grounded in the physiological body. We can see this understanding of the body in fields like psychopharmacology, in neurobiological treatments for trauma, and in the study of TBI.
We also see it in the focus on the vagus nerve, or the relationship between the size of the hippocampus and traumatic memories, or the function of the amygdala in PTSD. It’s also key to how we understand the relationship between dopamine and addictive behaviors.
The physiological body is “universal”: that is, it is said to work in the same way, across all people, throughout time. Treatment interventions based on the physiological body are given the most scientific credibility, as they hew most closely to the medical model.
The somatic body

Pexels—Image by Cottonbro
Interventions that focus on the body’s states of arousal, tension, movement, and breath are addressing what I’m calling the “somatic body.” Somatic treatments depend on the idea that we can regulate our states of arousal, and that this regulation will impact our ability to focus, to make decisions, to feel powerless or centered.
Practices like yoga, biofeedback, forest bathing, breathing, stretching and other forms of movement are designed to address the body by responding to the information it’s giving us. These practices help us attune to the fact of our embodiment and then do something to change it, or notice it, or work with it.
Somatic interventions often move away from questions of meaning-making, narrative, or unconscious exploration, in order to focus on the way our embodiment is experienced in the present moment, and the feelings, both emotional and physical, that we perceive. Even those interventions like meditation that also include attention to thoughts do so not to engage in the content of consciousness, but rather to notice the thoughts as effects of the body’s state.
Like the physiological body, the somatic body is universal: the interventions that focus on somatic responses are said to operate in the same way, and to have very similar impacts on the bodies of all people who engage in these practices.
The situated body
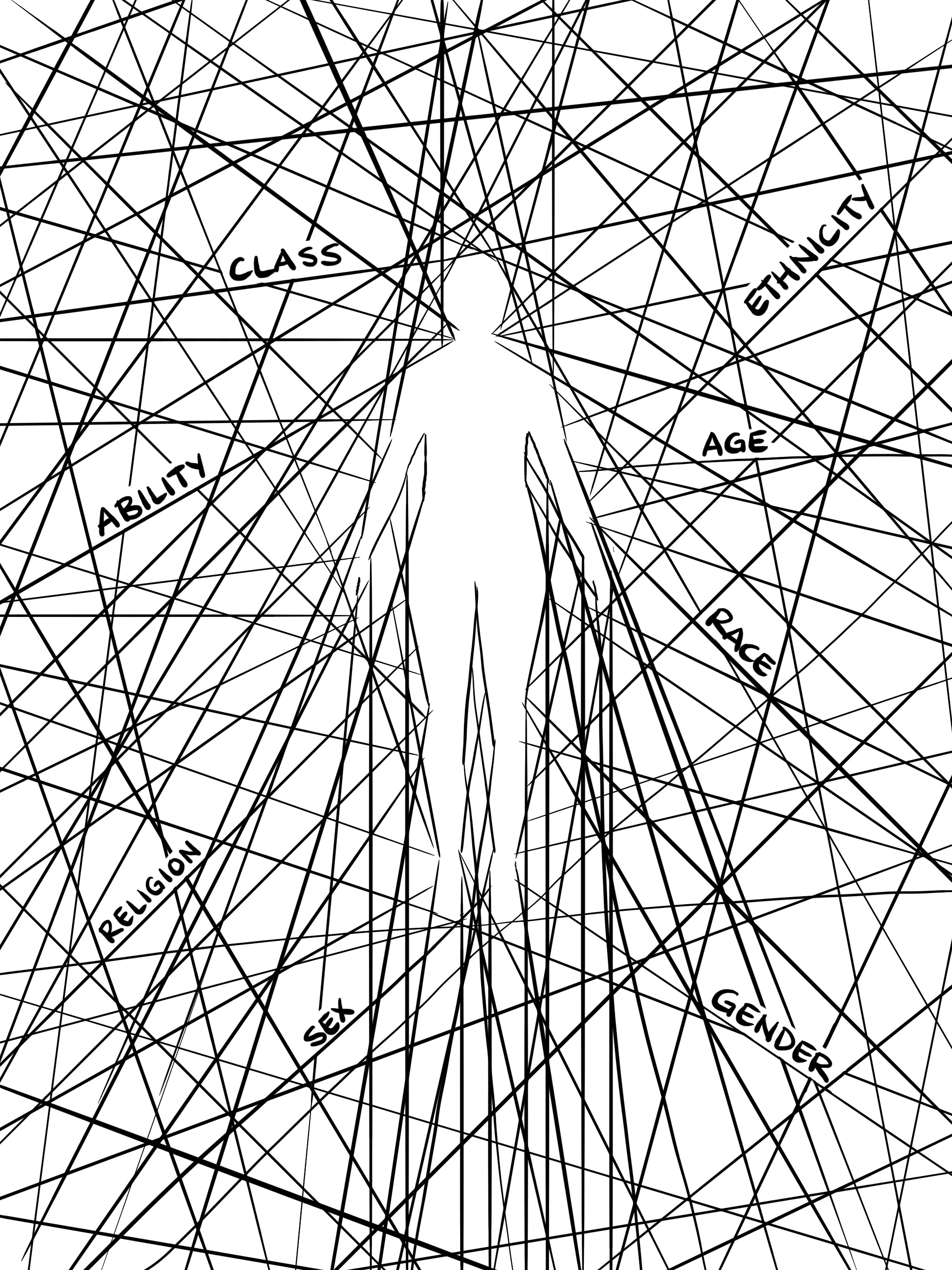
Image by Stef Koehler
In contrast to the two universal definitions of the body we’ve just addressed, the situated body is particular and specific: it says that how we come to know ourselves and our experience of embodiment is inextricable from our identities, our cultures, our geographical locations, our generational histories.
In this understanding, our body both registers our experiences and is shaped by the cultures in which it is situated. We come to know our bodies through the networks of structural violence and oppression that shape and impact them, and by the dominant culture’s representation of what a worthy or denigrated body is and looks like. We may also inhabit subcultures and families that resist these definitions, teaching us to experience our bodies as sources of resilience and wonder.
We come to recognize and name our bodies through language, which is an effect of culture. Our body, our flesh, our physiology and soma are made sense of through a language (or languages, if we speak more than one) that existed before us, and that we use to identify our being, our loves, our joy and despair.
Our body is also situated in terms of our relationship to power. It is represented in the dominant white culture as belonging to a phenotype that exists in a racialized schema, which influences how our body is received and made meaning of by ourselves and others. Our body is received by others as gendered, as raced, as classed, as signifying our ability, as aged, and the ways we are received may or may not match our internal sense of our own embodiment.
Many of the mainstream approaches to mental health treatment deny the specifics of the situated body and the ways our experience of embodiment, power, and oppression are present in our experiences of anxiety, or trauma, or depression. Most evidence-based practices are rooted in a universal definition of the body and thus presume that what anxiety “is” is stable and consistent across all people: that these terms are static—universal in the way they are understood, and uniform in the way they are experienced. But when we put the lens of the situated body over a term like anxiety, or trauma, or depression, these ideas become more complex, and we can ask what it might mean to include the situated body in all forms of mental health treatment.
When I sit with these three different definitions of embodiment, it makes me wonder: is there a way to access our embodiment outside of language? When we have a sensation and know that sensation in our body, is that sensation present to us through words? Through images? Through feeling? Is there a way to feel and be in our bodies that is “outside” or “before” a cultural meaning system of embodiment?
When we talk about trauma as registered in and through the “body,” are we talking about the ways bodies have been traumatized throughout history, and how that historical trauma is registered in the body in the present moment? Are we talking about the way the amygdala is scanning and responding to a perceived threat? Are we talking about our breath, trapped in our throat, and the way our heart races? Are we talking about the ways we have lived in a body the law tells us is not ours to control, that is subject to the whims and power of another? Are we talking about being in a body that feels like it has its own ways and wants, and that is unruly and disobedient and hates us?
I’d love to hear your thoughts on these questions in the comments on this post. I’d love to hear more about your practice, and which definitions of the body you use the most with your clients. I’d love to hear about your own experiences of healing, and being healed, and how you make sense of your own being, your own body.









Share this post